
Core Knowledge: Pelvic Fractures
03/09/14 11:47 Filed in: Core Knowledge
Pelvic Fractures

Today’s Wednesday Blog gives an overview of pelvic fractures, a common exam and interview question.
Background
Pelvic fractures account for approximately 3% of all fractures
They are due either to high energy injury, e.g. RTA’s and also low energy pubic rami fractures in the osteoporotic elderly population
Deforming forces on the injured pelvis come from 3 vectors:
AP
Lateral Compression (most common)
Vertical shear
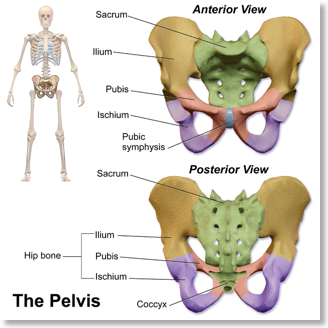
Anatomy
The pelvis is composed of the the hip bone (Ilium, pubis and ischium) and sacrum and coccyx. In trauma, due to it’s structure the pelvic ring can open at the front (the pubic symphysis) as in an open book fracture or at the SI joint at the back. Fractures tend to break the pelvic ring in two places and the close proximity of venous beds and arteries means that blood loss can be drastic.
BOAST Guidelines
The BOAST 3 Guidelines helpfully summarise the current literature and agreed management pathways for the management of pelvic trauma in the United Kingdom.
The guidelines themselves can be broken down into their constituent sections to aid learning:
- 1-3 ATLS
- 4-6 Urology
- 7-9 Definitive fixation
- 10-13 Acetabular fractures
Assessment and Immediate Care
ATLS Principles
Detection and treatment of life-threatening injuries
Haemodynamic instability (bleeding into free space)
- Posterior pelvic venous plexus (80%), superior gluteal artery or internal/external iliac branches
- Immediate control with pelvic binder or sheet
- Permissive hypotensive resuscitation
- Non-responders MTP RBC:PLTs:FFP 1:1:1ratio
- Look for bruising & haematoma
AP Pelvis and Assess for associated injuries:
Major urological injury 5-10%
- Blood at urethral meatus
- Difficulty passing catheter
Open Fractures <5%
- Examine perineum & PR
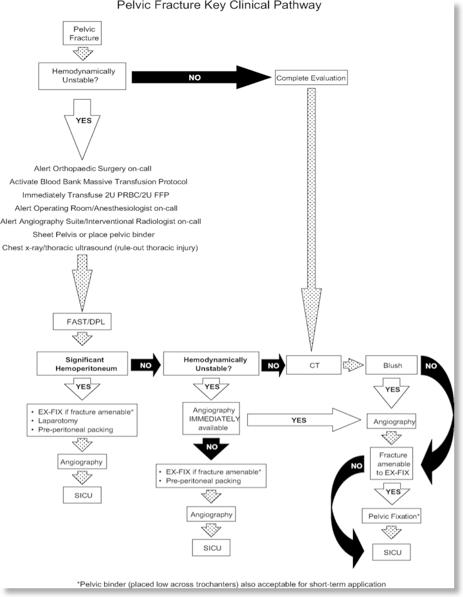
Management
BOAST 3 Summary:
ATLS
Haemodynamically stable → CT
If Unstable
- FAST/DPL if available in ED
- Angiography/Pre-peritoneal packing/Laparotomy
Urological Injury
- CT Urethography +/- cystography
- Early involvement of Urologists
Open fracture
- Urology and general surgery input for bladder drainage and potential colostomy
Definitive Pelvic Fixation in Specialist Unit within 5 days
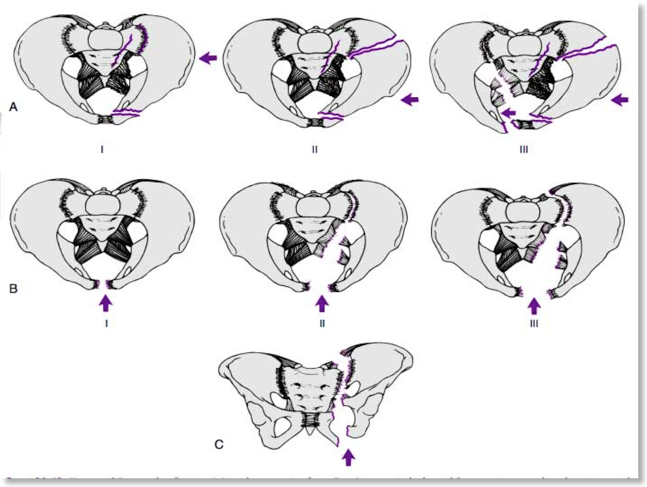
Classification
The Young & Burgess classification helps to guide management of pelvic fractures based on mechanism of injury
Lateral Compression (LC)
Type I: a posteriorly directed force causing a sacral crushing injury and horizontal pubic ramus fractures ipsilaterally. This injury is stable
Type II: a more anteriorly directed force causing horizontal pubic ramus fractures with an anterior sacral crushing injury and either disruption of the posterior sacroiliac joints or fractures through the iliac wing. This injury is ipsilateral
Type III: an anteriorly directed force that is continued and leads to a type I or type II ipsilateral fracture with an external rotation component to the contralateral side; the sacroiliac joint is opened posteriorly, and the sacrotuberous and spinous ligaments are disrupted
Anterior Posterior Compression (APC)
Type I: an AP-directed force opening the pelvis but with the posterior ligamentous structures intact. This injury is stable
Type II: continuation of a type I fracture with disruption of the sacrospinous and potentially the sacrotuberous ligaments and an anterior sacroiliac joint opening. This fracture is rotationally unstable
Type III: a completely unstable or a vertical instability pattern with complete disruption of all ligamentous supporting structures
Vertical Shear
The Tile classification is based on fracture stability:
Type A - stable
A1 – #s of the pelvis not involving the ring
A2 – minimally displaced #s of the ring
Type B – rotationally unstable, vertically stable
B1 - Open book
B2 – lateral compression: ipsilateral
B3 – lateral compression: contralateral
Type C – rotationally and vertically unstable
C1 – Unilateral vertical instability
C2 – Bilateral – both sides vertically unstable
C3 – Associated with acetabular fracture
Further Info:
For further info and examples of pelvic fractures and questions be sure to sign up to the Question Bank.