
Core Knowledge: Hip Approaches
02/10/13 03:53 Filed in: Core Knowledge | Wednesday Blog
Today’s Wednesday Blog gives an overview of approaches to the hip that you may be asked about at interview.
The best way to remember approaches and provide interviewers with a personalised answer is to get into theatre and perform or assist with the below operations. Writing out the steps or photocopying op notes can also help you to remember. Most candidates will have performed an antero-lateral approach and performed or seen a posterior approach and these are the most commonly tested approaches.
Antero-Lateral Approach (Modified-Hardinge or Watson-Jones)
Indication
Exposure to hip joint
Trauma THR, Elective THR, Hemiarthroplasty
Positioning
Patient on side in blocks
Anaesthesia & Abx
GA
Abx at induction
Intermuscular Plane
Tensor Fascia Lata (TFL) supplied by superior gluteal nerve
Gluteus Medius supplied by superior gluteal nerve
Risks
Superior Gluteal nerve (supplies abductors) 3-5 cm above GT
Skin Incision
10-15cm incision centred over tip of greater trochanter, 2/3 anterior to GT, 1/3 posterior
Superficial Dissection
Incise subcutaneous fat feeling for GT and femur and stay in line as you dissect down
Insert self-retainer to maintain tension on tissues
Below s/c fat is thick band of fascia lata, incise this with dissection scissors or blade
Clear bursa from muscle layer
Deep Dissection
Visualise abductors, ask assistant to externally rotate and abduct leg to put tissues under tension
Detach abductors from GT with cutting diathermy (an alternative is to perform a trochanteric osteotomy)
Expose capsule and perform T-shaped or straight capsular incision
Dislocate Hip
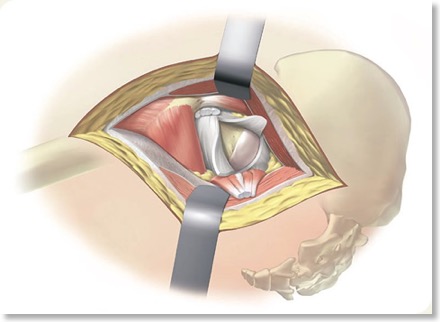
The hip joint will now be exposed.
Closure
2 vicryl to repair abductors
2 vicryl to repair fascia lata
2-0 vicryl to subcutaneous tissue
3-0 monocryl or clips to skin
Posterior Approach (Moore)
Indications
Elective THR
Positioning
Pt on side in lateral position in blocks
Anaesthesia & Abx
GA
Abx at induction
Intermuscular Plane
Split fibers of gluteus maximus supplied by inferior gluteal nerve
Risks
Sciatic nerve
Skin Incision
15 cm curved incision over posterior aspect of greater trochanter beginning 7cm superiposterior to GT and curving over GT then down femur
Superficial Dissection
Incise subcuatneous fat to fascia lata
Incise fascia lata to reveal vastus lateralis distally and gluteus maximus proximally
Split fibres of gluteus maximus and cauterise bleeding vessels (as this is a very vascular area)
Deep Dissection
Have assistant internally rotate the hip to put tension on the short external rotators
Place a stay suture in piriformis and obturator internus tendons (short external rotators)
Incise and detach piriformis and obturator internus from their femoral attachment and reflect backwards to protect the sciatic nerve
Feel for acetabulum and incise capsule with straight or T-shaped incision
Dislocate hip
The hip joint is now exposed
Closure
Repair short external rotators with stay suture
2 vicryl to TFL
2-0 vicryl to subcutaneous fat
3-0 monocryl or clips to skin
Anterior Approach (Smith-Peterson or Iliofemoral)
Indication
Minimally invasive surgery (MIS), pelvic osteotomy, biopsies and hemiarthroplasty
Positioning
Patient supine
Routine prep & drapes
Anaesthesia & Abx
GA
Abx at induction
Internervous Plane
Sartorius and Rectus Femoris supplied by femoral nerve
Tensor fascia lata (TFL) and Gluteus Medius supplied by superior gluteal nerve
Risks
Superior Gluteal nerve (supplies abductors) 3-5 cm above GT, lateral femoral cutaneous nerve
Skin Incision
Incision from anterior half of iliac crest to ASIS
Superficial Dissection
Identify internervous plane between sartorius and TFL
Dissect through subcutaneous fat
Incise fascia through medial side of TFL
Detach origin of TFL
Ligate ascending branch of lateral femoral circumflex artery
Deep Dissection
Identify internervous plane between rectus femurs and gluteus medius
Detach rectus femoris from both its origins
Retract rectus femoris and iliopsoas medially and glteus medius laterally
Adduct and externally rotate the hip to create tension on the capsule
Feel for acetabulum and incise the capsule with a longitudinal or T-shaped capsular incision
Dislocate the hip with external rotation once capsule released
The hip joint will now be exposed
Closure
2 vicryl capsular repair
2 vicryl to rectus femoris
2-0 vicryl to subcutaneous tissue
3-0 monocryl or clips to skin
Direct Lateral Approach (Hardinge)
Indications
THR, Trauma THR, Hemiarthroplasty
Positioning
Pt on side in blocks
Anaesthesia and Abx
GA
Abx at induction
Intermuscular Plane
No true plane
Risks
Superior Gluteal nerve (supplies abductors) 3-5 cm above GT
Skin Incision
15cm longitudinal incision centred over greater trochanter
Superficial Dissection
Incise through subcutaneous fat to fascia lata using self-retainer to keep tissues under tension
Split fascia lata with scissors or blade
Brush aside bursa from underlying abductors
Deep Dissection
Cutting diathermy through fibres of gluteus medius leaving a cuff for repair
Extend inferiorly through fibres of vastus lateralis
Incise and detach insertion of gluteus medius from anterior greater trochanter
Feel for acetabulum and perform straight or T-shaped incision into capsule
Dislocate hip
The hip joint will now be exposed.
Closure
2 vicryl to abductors
2 vicryl to TFL
2-0 vicryl to subcutaneous fat
3-0 monocryl or clips to skin
Further Resources:
AO Guide to Hip Approaches
Anatomy Resources: