
Core Knowledge: Calcaneal Fractures
18/09/13 08:14 Filed in: Core Knowledge | Wednesday Blog

Today’s Wednesday Blog is the first of many Core Knowledge topics aimed at potential Clinical Scenario questions that may be asked at Orthopaedic ST3 Interviews. This week we look at Calcaneal Fractures...
Overview
Most Frequent Tarsal fracture (60%)
75% intra-articular (subtalar), 17% open
- Mechanism: Fall from height, RTC
- Associated Injuries:
- Extension to calcaneocuboid joint 60%
- Vertebral injuries 10%
- Contralateral calcaneus 7-10%
- Prognosis: 40% complication rate
Anatomy
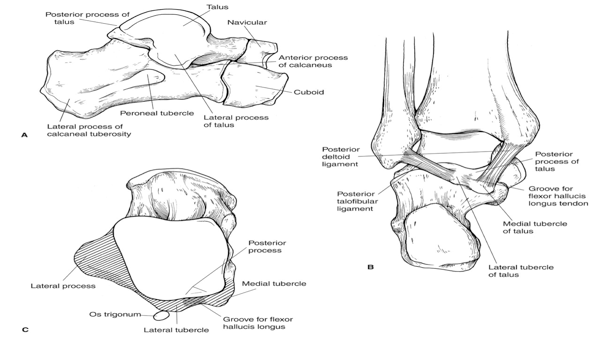
3 facets articulate with the talus:
- Posterior: majority of wt-bearing
- Middle: on sustentaculum tali
- Anterior: confluent with middle
Imaging
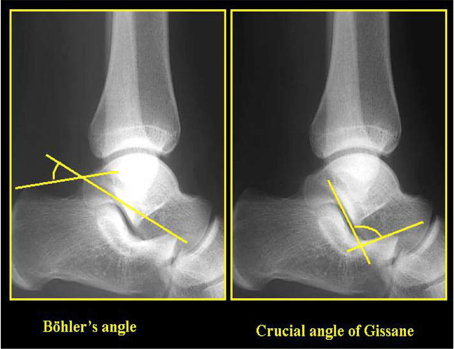
- Bohler’s angle (20-40) reduction indicates collapse of posterior facet
- Angle of Gissane (130-145) increase indicates collapse of posterior facet
- CT gold standard
Classifications
Anatomical (Extra and Intra-articular), Sanders (based on CT) and AO.
Extra-articular (25%)
- avulsion injury of
- anterior process by bifurcate ligament (below right)
- sustentaculum tali
- calcaneal tuberosity (below left)


Extra-articular fractures: Tuberosity (left) and anterior process (right)
Always consider anterior process avulsions in the differential diagnosis of the "sprained" ankle that fails to settle. It is usually seen on an oblique radiograph of the foot but may need a CT for diagnosis. Petrover et al (2007) found that 60% had calcaneonavicular coalitions and 69% bifurcate ligament sprains.
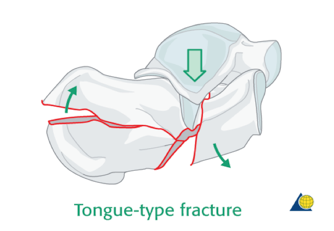
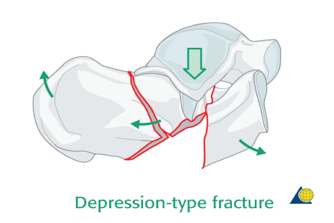
Intra-articular (75%) Essex-Lopresti Classification (1952)
- Primary fracture line runs obliquely through the posterior facet forming two fragments
- Secondary fracture line runs in one of two planes
- Tongue-Type: Exits posteriorly
- Joint Depression: Exits behind the posterior facet dissociating facet from tuberosity
Sanders Classification
- Based on the number of articular fragments seen on the coronal CT image at the widest point of the posterior facet
| I | Undisplaced posterior facet (regardless of number of fracture lines) |
| II | One fracture line in the posterior facet (two fragments) |
| III | Two fracture lines in the posterior facet (three fragments) |
| IV | Comminuted with more than three fracture lines in the posterior facet (four or more fragments) |
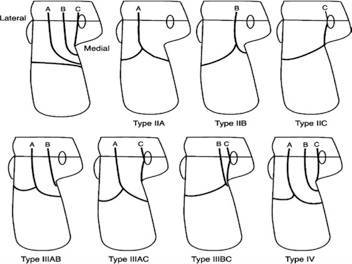
Sanders classification is based on CT findings and location of fracture lines. A-C subdivisions represent the position of the fracture lines.
Management
- Operative vs non-operative controversial
- Cochrane review 2013: 4 RCTs (620 pts)
- Buckley 2002 Canada 424 pts
- No significant difference in function
- Higher complications surgery, higher subtalar OA conservative
- Operative indications: displaced posterior facet, open fractures, calcaneocuboid >25%
- Most important factor is patient selection due to complications of surgery
- Conservative: Cast immobilisation, non-weight bearing 8-12 weeks
- Operative: ORIF with calcaneal plate via lateral incision to restore joint congruity
Complications
- Wound dehiscence: RFs BMI, open fractures, diabetes, smoking, male
- Chronic pain: RFs work-related injury
- Compartment syndrome: 10%
- Subtalar/calcaneocuboid OA
- Stiffness: 50%
- Increased heel width
- Mal/Non-union
- Sural neuropathy: lateral approach
Check back next week for more knowledge topics...